Assessment of locomotive syndrome among older individuals: a confirmatory factor analysis of the 25-question Geriatric Locomotive Function Scale
Abstract
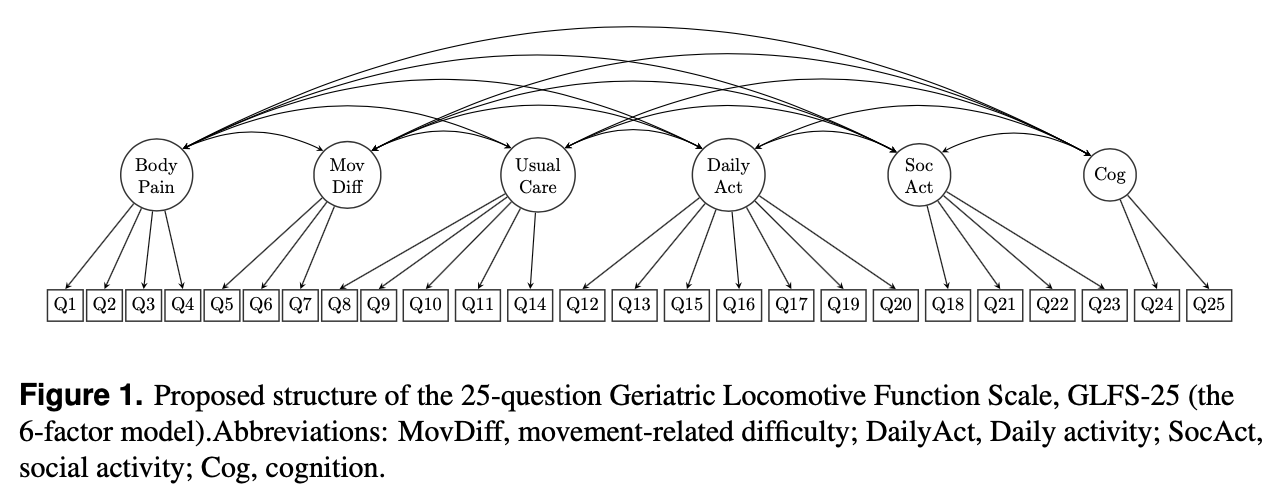
Background. The 25-question Geriatric Locomotive Function Scale (GLFS-25) is widely used in daily clinical practice in evaluating locomotive syndrome (LS). The questionnaire contains 25 questions aiming to describe 6 aspects, including body pain, movement-related difficulty, usual care, social activities, cognitive status, and daily activities. However, its underlying latent factor structure of the questionnaire has not been fully examined so far.
Methods. Five hundred participants who were 60 years or older and were able to walk independently with or without a cane but had complaints of musculoskeletal disorders were recruited face to face at the out-patient ward of Aichi Medical University Hospital between April 2018 and June 2019. All participants completed the GLFS-25. Confirmatory factor analysis (CFA) models (single-factor model, 6-factor model as designed by the developers of the GLFS-25) were fitted and compared using Mplus 8.3 with a maximum likelihood minimization function. Modification indices, standardized expected parameter change were used, standard strategy for scale development was followed in the search for an alternative and simpler model that could well fit the collected data. Cronbach’s $\alpha$ and its 95% confidence interval (CI) were also calculated.
Results. Mean (standard deviation) participants age was 72.6 (7.4) years old; 63.6% of them were women. Under the current criteria, 132 (26.4%) and 262 (52.4%) of the study subjects would be classified as LS stage 1 and stage 2, respectively. Overall, the Cronbach’s $\alpha$ for GLFS-25 evaluated using these data was 0.959 (95%CI: 0.953, 0.964). The single- and 6-factor models were rejected due to poor fit. The alternative models with either full 25 questions or a shortened GLFS-16 were found to fit the data better. These alternative models included three latent factors (body pain, movement-related difficulty, and psycho-social complication) and allowed for cross-loading and residual correlations.
Discussion. The findings of the CFA models provided evidence that the factor structure of the GLFS-25 might be simpler than the 6-factor model as suggested by the designers. The complex relationships between the latent factors and the observed items may also indicate that individual sub-scale use or simply combining the raw scores for evaluation is likely to be inadequate or unsatisfactory. Thus, future revisions of the scoring algorithm or questions of the GLFS-25 may be required.